Hi I’m Alyssa, and I’m creating the food allergy blog I wish I would have been able to follow while I was growing up. I am a 22 year old graduate student from Plymouth, Michigan and recently graduated from The Ohio State University. I am now pursing my masters in Counseling Psychology in Chicago, Illinois.
With a seemingly endless list of allergens that always served as my “fun fact” on the first day of school, I’ve decided to share my experiences, recommendations, tips and tricks with others managing severe food allergies too.
Having to avoid peanuts, treenuts, shellfish, chickpeas, raw eggs, raw tomatoes, apples, bananas, cantaloupe and honeydew has not been easy, but I haven’t allowed my allergies to restrict me from trying new and fun restaurants, eating fancy desserts, flying commercial airlines, traveling across country or living my life normally.
Whether it’s you or a loved one managing food allergies, I hope you find this blog helpful for restaurant recommendations, traveling hacks, allergy-friendly brand suggestions, and a place to share stories to keep each other safe.
What an incredible honor to share that I have successfully defended my doctoral dissertation, and received an award for my poster dissemination at our Graduate Research Forum!
My research, titled, Lived Experiences of Food Allergic Young Adults in Differentiating Anxiety from Anaphylaxis in the Aftermath of a Severe Allergic Reaction, has been such a labor of love over the past four years – And is now available online for public review! You can search for the full publication on ProQuest (ISBN:9798291582060), or download the PDF version below.
Take a look at the abstract from Bauder, 2025:
The physiological and psychological distress symptoms associated with anxiety are markedly similar to those seen in anaphylaxis, making it difficult to differentiate between the two acute reactions (Manassis, 2012). Research suggests that medically traumatic events like anaphylaxis have the potential to perpetuate brain-body disconnections (e.g., decreased interoceptive accuracy, increased sensitivity to interoceptive signals) that make it increasingly challenging to differentiate the overlapping symptomatology (Schaan et al., 2019; Manassis, 2012; Joshi, Aupperle, & Khalsa, 202). The misinterpretation of anxiety symptoms as medical emergencies is a well-known phenomenon in healthcare and emergency medicine, but has yet to be specifically explored in the context of food allergy. This study employed a mixed-methods research design to explore the functional impact of posttraumatic stress symptoms (PTSS) on survivors of food-induced anaphylaxis. The study gathered allergic disease and mental health data from twenty (n=20) food-allergic young adults. 65% of participants (n=13) reported that sometimes they cannot differentiate between anxiety and anaphylaxis symptoms. Five (n=5) participants who endorsed PTSS were further interviewed. Common themes across their interviews captured a shared lived experience of anxiety while attempting to authenticate anaphylaxis symptoms. It is the hope that the results of this investigation will provide healthcare professionals with a greater understanding of the psychological impacts of anaphylaxis and contribute to the future development of evidence-based prevention strategies and/or treatment protocols to alleviate undue psychosocial burden in this community.
My younger self, struggling to make sense of the impact an allergic reaction could have on her mental health, would be so proud to know that the ‘Anxiety or Anaphylaxis?’ phenomenon now holds a permanent place in the academic literature – Not only validating her personal experiences, but reassuring others that they are not alone.
It has been such an honor and a privilege to have the opportunity to amplify the voices of those in our community who have long suffered the psychosocial burdens of allergic disease.
This is just the beginning of an exciting career to come!
On April 26th 2025, my husband and I tied the knot in a celebration 4,376 days in the making!
Back in our home state of Michigan, our day was surrounded by friends, family, and loved ones. Noticeably absent from the guest list? Any and all nuts. Even though I grew out of my tree nut allergies at 25, I was adamant about having an entirely nut-free wedding – Just based on principle!
And I wanted that same peace of mind for my guests, too. Of our 140 guests, approximately 10% had food allergies and/or dietary restrictions – Which is on par with the national average for adults! So we made it a priority to accommodate each and every one of our guests – And from All Things Allergies, I hope they expected nothing else!
But we all know that food allergies are about so much more than “just” food. Our allergy-conscious wedding planning went far beyond simply selecting a safe menu – It required careful consideration of cross contamination, labeling, logistics, and more. Tying The Knot is a glimpse into the lengths we went to ensure a memorable, safe, and allergy-conscious wedding for ourselves and for our loved ones.
Choosing a Venue
Not only was Planterra Conservatory was the most beautiful backdrop for our wedding day, but we could not have been in better hands. Their award-winning botanical garden and next-level customer service was second to none. Because Planterra had mastered the big picture, we got to focus our attention on all of the little details that would make our celebration special. From writing “Peanut Free Menu. Bride is Severely Allergic. Check Oils.” on all of our contracts, to sending us off at the grand exit with bags full of leftovers, I simply cannot imagine having exchanged our vows anywhere else.
Collecting RSVPs
We designed our invitations and collected our RSVPs online through The Knot, where guests were able to list their dietary restrictions and preferences. I exported the information into an Excel file that could easily be shared with our venue and caterers. This method also helped us coordinate the vendor meals – Several of which were gluten free and dairy free.
Welcome Bags
For the guests staying at our hotel block, we had small welcome gifts for them upon arrival. The bags had an itinerary for the weekend, plus some local Michigan favorites – Vernor’s Ginger Ale, Sanders Caramels, and BetterMade Chips from a dedicated nut-free facility. For the two parties with milk allergies, we gifted them dairy-free Sanders dark chocolates.
Emergency Kits
In addition to the wedding day emergency kit with all my bridal essentials, we created an allergy-specific emergency kit with multiple EpiPens, allergy pills, Benadryl cream, and Well Too Wipes. We tucked it under the Sweetheart Table to ensure it was easily accessible during dinner without being an eye sore! Our bridal party and the wedding coordinator knew where it was in the event of an emergency.
Pre-Ceremony Snacks
Since I first came across Thyme and Honey, I knew I needed to find a way to incorporate them into our wedding weekend. We ordered grazing boards for our bridal party and family to enjoy during portraits. This was the perfect, bite-sized snack to keep my energy levels and blood sugar up throughout the busy day – And to my delight, the charcuterie was delivered with accompanying “NUT FREE” labels.
Walking Down the Aisle
No, we didn’t hire an allergy-friendly string trio to play our ceremony music – But my song choices were certainly inspired by my life experiences with allergies. Some of my fondest childhood memories are from family vacations to Disney World – Largely due to the way the chefs would go above and beyond to take care of me and my food-allergic brother at the parks. So, it should come as no surprise that Can You Feel The Love Tonight? holds a very special place in my heart and made for a beautiful moment as my dad escorted me down the aisle. Isn’t it fascinating the way allergies can shape our lives?
Catering
One of the deciding factors when booking Planterra Conservatory as our wedding venue was the allergy-conscious nature of their catering team. Planterra partners with Continental for in-house food and beverage services – And we were very impressed with their protocols for handling dietary restrictions, including helping us craft an entirely nut-free menu. I had specifically asked for the servers to be knowledgeable of any top nine allergens in each dish, especially when passing around hors d’oeuvre during cocktail hour.
About two weeks out from our wedding day, I submitted a color coordinated seating chart to the catering team outlining our guests dietary restrictions. In combination with the table setting procedure shown below, Continental seamlessly coordinated safe food service for all of our guests.
Table Settings
Because so much of the food allergy experience is characterized by exclusion and othering, I wanted our wedding to be a place where allergies were not just accommodated, but celebrated. So to help the servers easily identify dietary restrictions at our reception, I added these gold wax seals only to the name tags of our guests with allergies. It was a minor detail – but it was a chance for the allergy kid to get something, instead of having something taken away.
Shown above on the customized menu, our three courses were also labeled accordingly as gluten-free (GF), dairy-free (DF), and nut-free (NF).
Wedding Cake(s)
We hired Sweet Heather Anne to design our wedding cake knowing the bakery did not use peanut products, and had a protocol for reducing cross contamination with tree nuts. We offered our guests two flavors – Chocolate Raspberry with Rose Buttercream or Lemon Cake with Strawberry Buttercream.
For our GF/DF guests, we had a third option. Sweet Heather Anne partners with another local bakery called Botanical Bakeshop – A 100% vegan bakery with gluten free accommodations. Botanical Bakeshop delivered their 15-slice cake to Sweet Heather Anne, who delivered both cakes to our venue on wedding day. No one is missing dessert at my party!
Bar Service
The allergy-friendly menu didn’t stop at food – Alcoholic beverages commonly contain allergens, too! We crafted three signature cocktails – The Columbus Strawberry Basil Margarita, the East Lansing Knob Creek Old Fashion, and the Chicago non-alcoholic Lavender Lemonade.
Cappuccino Bar
To keep the energy up on the dance floor, The Cappuccino Man brewed late night coffee for our guests, topped with custom latte art of our beloved Alma Maters. The Cappuccino Man was more than happy to thoroughly sanitize all of their equipment, and leave the almond milk, pistachio syrup, and hazelnut creamers off the menu.
Floral Design
Despite the year and a half of wedding planning, I suppose there’s some things you just cannot plan for… While our floral arrangements were unbelievably beautiful, it turns out my groom was allergic! On his first day married to All Things Allergies, Connor broke out in full body hives after helping carry the bouquets home from the venue – Thankfully he did not suffer any symptoms until after the big day! After Zyrtec and antihistamine cream failed so stop the reaction, we headed to urgent care for a prednisone injection.
My better half is good as new now and ready to schedule his first allergy appointment – What are the odds?!
To add insult to injury, my seasonal congestion turned into a sinus infection this fall – And after ten days of symptoms, I was prescribed a round of antibiotics from my local urgent care.
Since breaking out in hives while taking Amoxicillin as a kid, I grew up under the impression that I was allergic to that class of antibiotics. For years, my doctors recommended Zithromax over Penicillin without hesitation.
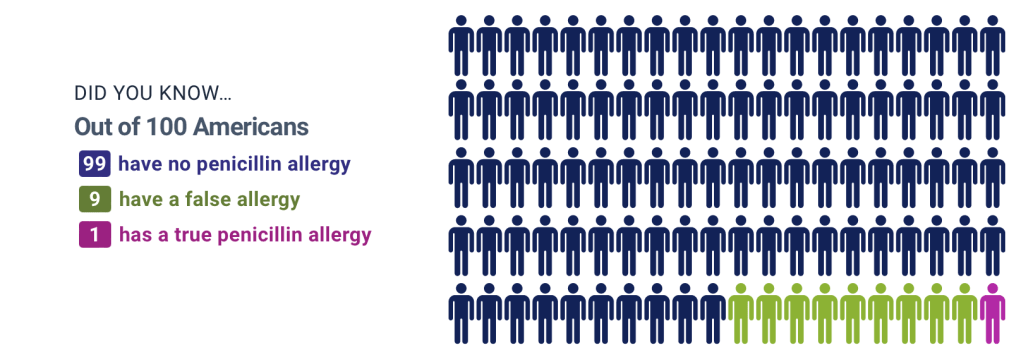
And I was in good company – According to Cincinnati Children’s Hospital, approximately 10% of Americans are labeled as having a Penicillin allergy.
But new research suggests that Penicillin allergies have been historically over-diagnosed, and the genuine rate of the allergy is closer to 1% of the U.S. population.
Courtesy of Cincinnati Children’s Hospital
What has led to 9 out of every 100 American to have a false Penicillin allergy? Dr. Sandy Durrani of Cincinnati Children’s offers a few possible explanations:
Rashes and hives are often misinterpreted as an allergic reaction to the medication, when “in reality, most commonly it is a virus” causing those symptoms.
Gastrointestinal symptoms – A common side effect of antibiotic medications – can also be misinterpreted as an allergic reaction.
A family history of Penicillin allergies can contribute to the misdiagnosis of this allergy.
Once “Penicillin Allergy”is added to someone’s medical chart, it is rarely challenged or reevaluated – Despite research that suggests 90% of individuals with a genuine Penicillin allergy will outgrow it within 10 years.
Healthcare professionals are hoping to raise more awareness of this public health issue because the alternative antibiotic prescriptions are often less effective, more expensive, and accompanied by worse side effects.
To determine if you have a genuine Penicillin allergy, an allergist can preform a skin prick and/or oral food challenge (OFC) to help make the proper diagnosis.
At my allergist appointment in 2021, Chicago Family Allergy & Asthma found that I was indeed one of the 90-95% of patients who were unnecessarily avoiding Penicillin products. I have since taken two rounds of the medication without issue.
The first prescription of Amoxicillin was rightfully blocked by my pharmacy, given that “Penicillin Allergy” was still listed in my chart – But with a quick update to my medical history, I’m now treating my sinus infections with the best antibiotic on the market.
Three cheers for modern medicine!
DISCLAIMER: The content of this post is for educational purposes only, and should not be substituted for medical advice. Please consult with your doctor for more information.
Why Severe Allergies May Disqualify You From Joining The United States Armed Forces
Did you know that having a life-threatening food allergy can disqualify you from joining the US Armed Forces?
To join the US Military, recruits must undergo a medical screening/examination to determine their eligibility and fitness for duty. According to the US Department of Defense Instruction, all recruits must meet the following criteria:
The person under consideration is free of contagious disease that will probably endanger the health of other personnel.
The person is free of medical conditions that required excessive time lost from duty for necessary treatment or hospitalization.
The person is medically capable of satisfactorily completing required training.
The person is medically adaptable to the military environment without the necessity of geographic limitations.
The person is medically capable of performing duties without aggravations of existing medication conditions.
Within the more specific medical standards, the US Department of Defense Instruction finds a “History of systemic allergic reaction to food or food additives” to be disqualifying medical condition from the US Armed Forces.
The rationale? Military service people are subject to be deployed to remote locations with limited food supplies and variable healthcare options. Further, cofactors known to decrease anaphylaxis thresholds are common to military life (e.g., fatigue, physical exertion) and may put the service person at increased risk for severe reaction.
In 2017, the Military Allergy and Immunology Assemble (MAIA) of the American Academy of Allergy, Asthma, and Immunology (AAAI) conducted a review of each military branch’s policies related to IgE-mediated food allergies. The US Army, Navy, Air Force and Marine Corps have different enlistment regulations and retention policies, summarized in this article from AAAAI.
Medical Waivers
Applicants with a disqualifying condition can request medical waivers/exemptions to clarify their eligibility. The following section highlights scenarios in which such waivers are likely to be granted or withheld for atopic conditions:
Unlikely to Receive Waivers
Applicants with a “history of systemic allergic reaction to food or food additives” are unlikely to be granted a medical waiver.
Applicants who are recommended by their military or civilian allergist to carry an epinephrine auto injector are unlikely to be granted a medical waiver.
Applicants who demonstrate IgE-sensitization and decline to conduct an oral food challenge are unlikely to be granted a medical waiver.
Applicants who demonstrate IgE-sensitization and fail an oral food challenge are unlikely to be granted a medical waiver.
Applicants diagnosed with eosinophilic esophagitis are unlikely to be granted a medical waiver.
Likely to Receive Waivers
Applicants who demonstrate IgE-sensitization, but successfully pass an oral food challenge without reaction, are likely to be granted a waiver.
Applicants with oral allergy syndrome are likely to be granted a waiver for this condition.
More Than Food
While All Things Allergies hopes to empower our community not to be held back by their chronic conditions, this is an admittedly disheartening reminder of the legitimate barriers imposed food allergy.
Food allergies have always been about more than food – Disqualification from the US Armed Forces is just another example of the systemic impact of allergic conditions on our educational, career, and lifestyle choices.
Waibel, K., Lee, A., Coop, C., Mendoza, Y., White, K. (2018). Food allergy guidance in the United States military: A work group report from the American Academy of Allergy, Asthma & Immunology’s Military Allergy and Immunology Assembly. Journal of Allergy and Clinical Immunology, Volume 142, Issue 1, 54 – 59. https://www.jacionline.org/article/S0091-6749(18)30705-X/fulltext
To have my updated allergy testing done, my allergist had me stop taking antihistamine medications prior to the appointment to ensure we were gathering the most accurate scratch test results. That week, I vividly recall struggling to fall asleep, kept awake by intense itching all over my body. I scratched so furiously that I left marks on my skin, unsure that I’d be able to tough it out until my upcoming clinic visit.
Surely it was all in my head, right? I just needed to stop thinking about it and the feeling would magically dissipate. Desperate for the unpleasantness to end, even talked with my therapist about how to practice putting my mind over matter.
Well, it seems I chalked up this debilitating itchiness to anxiety a little too quickly, as research suggests that there may have been a physiological explanation for my discomfort.
Cetirizine, a second-generation antihistamine sold under the brand name Zyrtec, is an over the counter medication used for 24-hour allergy relief from hay fever and hives. Antihistamine medications like Zyrtec relieve allergy symptoms by blocking histamines from attaching to H1 receptors in the body, disrupting the inflammatory response.
Zyrtec is considered safe for daily consumption, but prolonged use of such antihistamine medications has been linked to an ironic side effect.
In 2017, the Food and Drug Administration (FDA) found that the sudden discontinuation of cetirizine may result in pruritus — Meaning that stopping Zyrtec cold turkey after more than 6 months of use can cause generalized itching! This side effect is harmless, but undeniably uncomfortable, and can take days to even weeks to fully subside.
So, the medication used to treat itchiness can actually cause itchiness?
It turns out this phenomenon is relatively common in medicine! Let’s use hangovers as an example.
Alcohol intoxication typically results in drowsiness and disinhibition, whereas alcohol withdrawal (e.g., sobering up) often leads to insomnia, irritability, anxiety, headaches, and a general sense of discomfort. It’s like a teeter-totter effect — As our bodies strive to regain balance, they can “overshoot” and produce these opposing symptoms.
Withdrawal symptoms can be alleviated by gradually weening yourself of the substance, allowing the body more time to adapt to the lowing dose. That’s where the phrase “Hair of the Dog” comes in. Feeling hungover? Having another drink might help ease your symptoms.
However, Zyrtec has not included a specific weaning schedule in their drug information. Board certified allergist, Dr. Rubin, suggests consulting with your doctor about how to best taper off the medication to avoid such side effects.
So, it turns out my mind might not have been playing tricks on me after all. For as often as I have to reassure my anxious brain that I’m not experiencing allergy symptoms, it was quite validating to learn that this case wasn’t just in my head.
Disclaimer
The contents of this article are intended for educational purposes only, and should not be substituted for medical or professional advice. Please contact a licensed medical or mental health professional for more information.
References
Chung, A. H., La Grenade, L., & Harinstein, L. M. (2019). Pruritus after discontinuation of cetirizine. Therapeutic Advances in Drug Safety, 10. https://pubmed.ncbi.nlm.nih.gov/31308927/
Northwestern Medicine’s Center for Food Allergy and Asthma Research (CFAAR) hosted their second annual Global Food Allergy Prevention Summit this past week in Chicago, Illinois – And I had the pleasure of attending this world class right in my own backyard.
The three day conference offered multiple tracks – including the Summit for Advancing Equity in Food Allergy (SAEFA), Pediatric Food Allergy Care Conference (PFACC), and the overarching Global Food Allergy Prevention Summit (GFAPS).
The conference welcomed primary care providers, allergy and immunology specialists, researchers, industry partners, and policy makers alike to discuss the future of allergic disease management. Patients and their families were also offered a seat at the table to contribute their perspectives alongside experts and thought leaders.
It was awe-inspiring and incredibly refreshing to witness such collaborative efforts among interdisciplinary professionals who all share a common goal – To prevent food allergy!
Indeed, the future of medicine lies in integrated healthcare.
The Center for Food Allergy and Asthma Research recognizes that the advancements in allergic disease prevention and treatment are not evenly distributed across the food allergy landscape, and while the new medication options and early introduction protocols on the horizon will do wonders for our community, we cannot allow them to create further disparity across this population.
The Summit for Advancing Equity in Food Allergy (SAEFA) agenda was dedicated to discussing health equity in food allergy prevention, diagnosis, treatment, and daily life – Hosting four panels of community members from a variety of expertise and backgrounds.
Health disparity is defined as, “A health difference that is closely linked with social, economic, or environmental disadvantage.” We know that race, ethnicity, gender, sexual identity, disability, socioeconomic status, and geographic location all contribute to an individual’s ability to achieve good health – But how does that manifest specially in food allergy?
Here were some of my key takeaways from our discussion:
With only 4,000 practicing allergists in the United States, and less than half of those accepting Medicaid insurance, many families do not have access to specialist care.
The majority of pediatricians + primary care providers do not feel comfortable diagnosing food allergies.
Consequently, only 0.6% of children enrolled in Medicaid have a food allergy diagnosis – Which is a gross underestimation of the actual burden, based on epidemiological data.
Poor health literacy is a major barrier to health equity. Providers need to avoid using medical jargon to ensure patients and families are obtaining, processing, and understanding the information offered to them.
WIC – the special supplement nutrition program for women, infants, and children – does not adequately offer food products necessary for early introduction – A practice we know is quite effective in the prevention food allergy.
While research like the FORWARD study is starting to explore racial differences in food allergy, there is virtually no data on allergic disease prevalence in the Native American population.
The Center for Food Allergy and Asthma Research plans to publish a journal article summarizing the collective efforts of GFAPS 2024, which will highlight these disparities and offer a road map for breaking down health equity barriers in food allergy.
As a patient, mental health professional, and social media advocate, my role at the summit was to give a voice to those who have already been diagnosed with food allergies at a conference largely dedicated to allergic disease prevention.
So, to speak up and speak out about #FoodAllergyMentalHealth, I presented my dissertation literature review and research proposal covering the psychosocial consequences of anaphylaxis + the overlapping symptomatology of anxiety and anaphylactic shock at the conference poster session.
What an incredible moment to see three years of hard work having its moment in the sun!
The summit came to a close along the Chicago River, as the CFAAR team hosted an evening boat tour + happy hour for the attendees. As we networked, danced, and watched the sun set over the cityscape, I felt incredibly grateful to have found myself amongst such a likeminded, passionate, and dedicated team of people.
Thank you Lurie Children’s Hospital, Northwestern University Feinberg School of Medicine, and the Center for Food Allergy and Asthma Research team for hosting this event.
Because of you, I have so much hope for the future!
“I’m just a bill, and I’m sitting here on Capitol Hill.”
I did a Schoolhouse Rock crash course before coming to Washington DC, and now I can’t get that song out of my head!
On May 8th, 2024, the Allergy and Asthma Network (AAN) hosted their 27th annual Allergy and Asthma Day on Capitol Hill – And I was honored to have been invited to join the non-profit organization’s efforts towards health equity on the federal level.
This Allergy and Asthma Awareness Month, AAN is advocating for ease of access to life-saving medications across the atopic community. When meeting with our local congressmen and women on Capitol Hill, we asked for their cosponsorship of the following five bills:
Safe Step Act: Improves health insurance step therapy protocols and ensures patients are able to obtain the best treatment prescribed for them.
Help Ensure Lower Patient (HELP) Copays Act: Requires health insurers to count the value of copay assistance toward deductibles or out-of-pocket maximums.
Epinephrine Pharma Inflated Price Ends Now (EPIPEN) Act: Caps out-of-pocket cost for a two-pack of epinephrine auto-injector devices at $60 for patients with employer-based or individually purchased health insurance.
Elijah E. Cummings Family Asthma Act: Expands the CDC’s National Asthma Control Program to all 50 states; directs the CDC to collaborate with state and local health departments on information and education to the public on asthma; requires the development of state plans around public health responses to asthma; and requires the collection and coordination of data on the impact of asthma.
Dillon’s Law: Incentives states to train, certify, and enable good Samaritans to give epinephrine to a person experiencing anaphylaxis in the event they need the medication before emergency medical services can arrive.
As constituents of the state of Illinois, my team met with the staff of Senator Richard Durbin, Representative Mike Quigley, Representative Robin Kelly, and Representative Danny Davis. It was such a privilege to have our voices and stories be heard in the nation’s capital.
While this proposed legislation would ultimately serve our entire community at large, the Allergy and Asthma Network’s advocacy work is specifically directed towards improving health equity and patient care for Black and Hispanic families living with these conditions.
Epidemiological research has identified significant health disparities for Black and Hispanic people living with asthma, atopic dermatitis, and food allergies. These communities are disproportionately affected by these diseases due to lower socioeconomic statuses, poor access to health care, and environmental injustices. The following statistics offer some context for the negative health and financial outcomes of these chronic diseases.
Food allergy prevalence is higher among Black children (7.6%), compared to white children (5.3%).
Black and Hispanic children are 2.3x and 2.8x more likely to experience anaphylaxis from food allergens.
Asthma prevalence is higher among Black (14.3%) and Hispanic (17%) children, compared to white children (5.6%).
Black people are 3x more likely to die from asthma.
Black and Hispanic families have greater difficulty filling their prescription medications due to high costs.
Statistics provided by Allergy & Asthma Network
Over the past decade, the allergy and immunology field has made great advancements in the diagnosis, treatment, and therapy of these chronic diseases – But the communities most in need of these interventions are the same communities with the poorest access to them.
The Christopher D. Redding Youth Asthma Foundation is doing something about that. The Redding family lost their youngest son, Christopher, at just 18 years old to an exercise-induced asthma attack. As an otherwise healthy college student and young multi-sport athlete, his death came as a significant shock amongst all their grief. His parents, Mr. Michael Redding and Mrs. Helen Hammond Redding, have made it their life’s mission to spread awareness and education about this condition in order to prevent undue tragedy in other families. The foundation that lives on in their son’s name is bringing asthma and allergy care to the underserved populations of Chicago. The Lake County Asthma Van has served almost 1,500 children through its state of the art mobile clinic. Driving school to school, the free of cost service is bringing the necessary care straight to the doorstep of the patients in need.
The Redding family traveled to Washington DC with the Asthma and Allergy Network to advocate for the Elijah E. Cummings Family Asthma Act, which is particularly aligned with their mission. It was an honor to have been partnered with Mr. and Mrs. Redding as we met with our shared Illinois representatives on Capitol Hill. Hearing their story throughout the day was repeatedly impactful, and I am so inspired by their continued strength, dedication, and grace.
Together, we can help support, protect, and advocate for our most vulnerable communities across the allergy and asthma landscape. If you would like to get involved, please go to the Allergy and Asthma Network Advocacy Page for more information.
As Someone with Severe Anxiety and Even More Severe Food Allergies
With just over a week until we jet off to Spain, I cannot help but lay awake at night and think about our upcoming seven hours of flight time over the Atlantic. My ruminating thoughts jump to what-ifs and worst case scenario thinking…
Until I reflect on all of the food allergy community members who have safely gone before me. Traveling internationally never felt like an option for my family, but watching The Hivey League bravely explore every corner of our planet has given me the confidence to do the same.
Airlines are already challenging enough to navigate with their inconsistent policies and lack of accountability, but adding a language barrier, in-flight meal services, and no room for an emergency landing adds a whole new layer.
So here’s what I’m doing to make sure I’m prepared.
+ Bag: The Béis Mini Weekender is the perfect sized personal item – Big enough to carry all of my stuff, but compact enough to fit under the seat.
+ Toiletry Bags: I could not resist snagging the matching Béis In-Flight Cosmetic Set to organize my toiletries. The clear plastic design makes it TSA approved!
+ Wipes: For wiping down my seat and tray table, I stocked up on standard Clorox wipes in addition to the WellToo Peanut Allergen Wipes. These are, without a doubt, the greatest invention ever.
+ ExtraCleaning Supplies: Each time I fly, I pack a set of nitrile gloves and a standard garbage bag in a quart-sized Ziploc. I throw on the gloves while I wipe down my seat, and put the dirties in the Ziploc afterwards. Before putting my personal item under the seat in front of me, I place it inside the garbage bag. Any weird looks I get from passengers is 100% worth the peace of mind knowing my belongings are safe from whatever lingers on the floor.
+ Auto Injectors: A minimum of two – Always! But I will slip a third pen from a different lot in my fiancé’s bag, just incase.
+ Masks: One perk of COVID-19 was the normalization of mask wearing. Not only will an N95 protect you from germs, but it offers a sense of safety from surrounding allergens, too.
+ Pill Case: My seven day organizer from Port and Polish stays in my carryon, just incase our checked luggage gets misplaced.
+ Air Tags: Speaking of lost luggage, we slip Apple AirTags into our carryons and checked bags for stemless tracking. If you purchase from Apple, you can also get free engraving!
+ Allergy Translation Card: The food allergy cards from Equal Eats can be translated into 50 languages! Who knew the Catalonian word for peanuts is cacauets?
+ Eye Mask: I’m banking on getting a few hours of Zzzs on our red eye, and the Slip Sleep Mask is my best chance.
+ Noise Cancelling Headphones: The Apple AirPods Max are perfect for pre-downloaded audiobooks, podcasts, and movies while I’m awake, and for drowning out the other passengers while I’m asleep.
+ Pillow and Blanket: Airline linens are not known for their high thread counts or high grade disinfectants. The Bleusalt Scarf is not only the softest staple piece for your capsule wardrobe, but it also doubles as a thin blanket at 10,000 feet. Because I don’t find the standard C-shaped neck pillows to be very comfortable, I’ll be trying out the Dot&Dot Twist Memory Foam Pillow from Amazon this time around.
+ Safe Snacks: I am not planning to eat the in-flight meal provided by United – That’s just too far out of my comfort zone at this point. Instead, I’ll be tiding myself over with 88 Acres Seed Bars and That’s It Fruit Bars until we land.
+ Hydration: Dehydration is a cofactor for anaphylaxis, so keep up with your water! I’m packing a screw top bottle so the mouthpiece stays clean and covered.
+ Skin Care: The high altitudes are notorious for drying our skin out, too! My toiletry bag will have all my gentle, hydrating favorites including CeraVe Lotion, Aquaphor Lip Repair, and Blink Lubricating Eye Drops.
+ Compression Socks: Maybe not the most stylish, but this best selling set from Amazon will get the job done.
Next Stop: Barcelona!
To all of you who have conquered this feat before me – What am I forgetting?
Not only does it stay on the lips of All Things Allergies, but the psychological and physiological similarities between the fight-or-flight response and food-induced anaphylactic shock is also the subject of my doctoral dissertation proposal.
Inspired by my own recovery from the Invisible Consequences of Anaphylaxis, this research has been both personally and professionally rewarding… My literature review continuously validating the lifelong experiences I used to suffer in silence.
The Hivey League has already established how challenging it is for us to differentiate between anxiety and anaphylaxis, but I recently came across some pretty powerful evidence that even trained medical professionals may have trouble making sense of the symptoms, too.
And this was certainly was not the first time a peer-reviewed journal article has brought me to tears… I’m on year three of a four-year homework assignment, after all. But this time was different, as if Google Scholar was speaking straight to first grade Alyssa when it said, “It’s not just you.”
In the state of Georgia, public health researchers investigated 79 reports of adverse postvaccinal events following a 2008 measles-rubella vaccination campaign. The team was tasked with investigating this collection of severe reactions to dissuade safety concerns and combat vaccine hesitancy.
Through their causality assessment, the researchers attributed vasovagal syncope and/or anxiety attacks to 37 of the adverse reactions. This was relatively unsurprising, given that needle phobias and dizzy spells are routinely seen by health care workers.
But what was surprising is that of those 37 cases that were retroactively identified as anxiety attacks, 97.3% were originally misdiagnosed as postvaccinal anaphylactic reactions. Nearly every single one.
If even trained medical professionals cannot effectively differentiate between anxiety and anaphylaxis symptoms, it’s no wonder that the traumatized food allergy community cannot either.
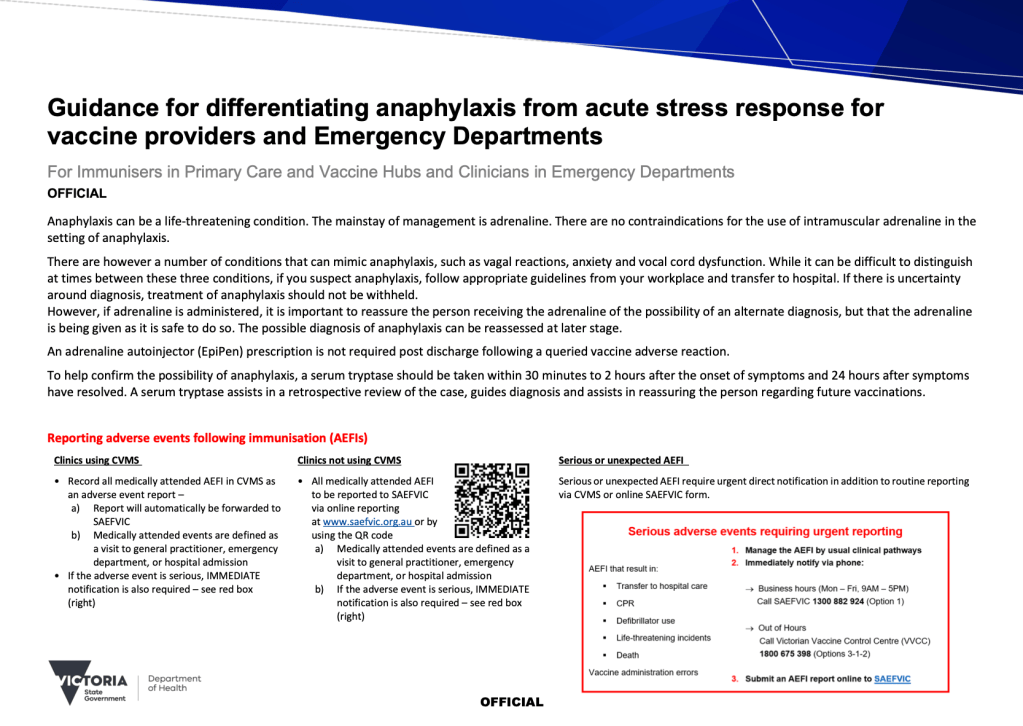
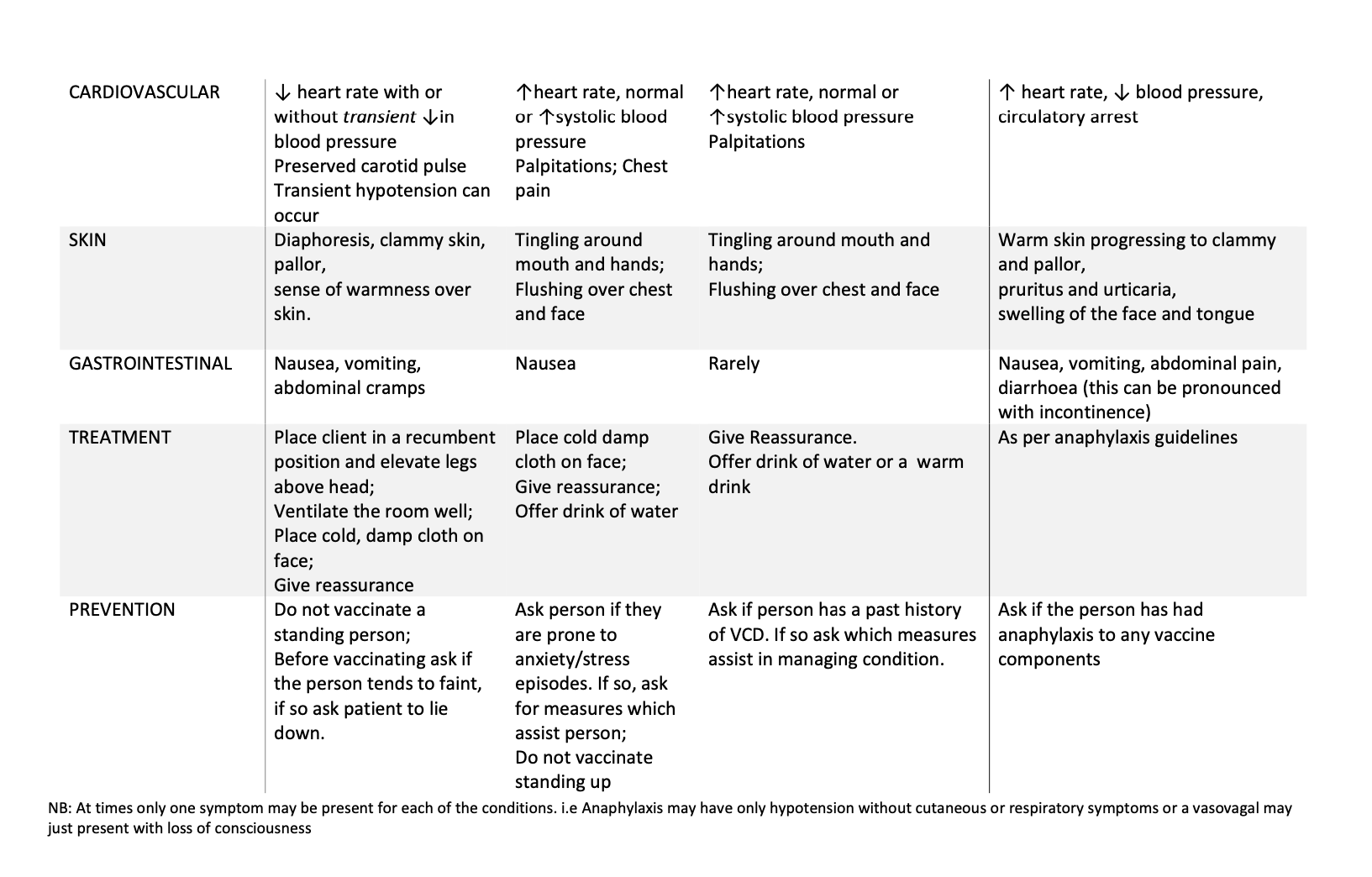
In Victoria, any reactions resulting from immunizations are reported to the Surveillance of Adverse Events Following Vaccination in the Community (SAEFVIC). The collection of this data has helped the Melbourne Vaccine Education Center offer an entire COVID-19 Vaccines and Allergy brochure, which includes a four-minute cartoon illustrating the difference between anaphylaxis and acute stress responses.
With these publications, the Anxiety or Anaphylaxis debate quickly went from a proposed hypothesis I would need to argue in my dissertation defense, to an established psychological phenomenon with a documented research backing. Of course this helped push along my literature review, but more than anything, it substantiated what I’ve known so long to be true.
I wasn’t going crazy. I wasn’t making it up. Whether it be food-induced, vaccine-induced, or otherwise, panic attacks undoubtedly mimic anaphylactic shock.
References
Khetsuriani, N., Imnadze, P., Baidoshvili, L., Jabidze, L., Tatishili, N., Kurtsikashvili, G., Lezhava, T., Laurent, E., & Martin, R. (2010). Impact of Unfounded Vaccine Safety Concerns on the Nationwide Measles-Rubella Immunization Campaign, Georgia, 2008. Vaccine (28), 6455-6464.
Melbourne Vaccine Education Centre. (2021). Guidance for Differentiating Anaphylaxis from Acute Stress Response for Vaccine Providers and Emergency Departments. Victoria Department of Health.
Disclaimer
The content of this post is for educational purposes only, and should not be substituted for medical or professional advice. Please consult with your doctor for more information.
Defining Immunoglobulin E, Debunking Antibody Myths, and Delving Into My Updated Bloodwork
“Another primary reason for misdiagnosis is a lack of understanding of what the results of serum IgE testing truly mean. In the absence of clinical IgE-mediated symptoms with ingestion of the food, a positive serum IgE test to that food merely means a patient is sensitized to it.”
Just two years ago, I had a life-changing appointment at Chicago Family Allergy and Asthma, walking into the routine check-up with a laundry list of severe food allergies and walking out with only one. Prone to passing out during blood draws, I had put off the visit for nearly five years – Why the sense of urgency if I wasn’t expecting to hear anything new? Well, my IgE levels certainly had a different idea in mind.
In my blog post, And Then There Was One, I detail the journey of how All Things Allergies nearly became All Things Allergy with the big reveal of my undetectable bloodwork. I remember answering the phone call with my results like it was yesterday, quickly cycling through the five stages of grief.
This cannot be right. I’m going back to the office for a confirmatory scratch test. Denial. Why didn’t I make this appointment earlier?! Anger. I should just keep avoiding them though, right? Bargaining. I feel like an imposter. Depression. Your body just offered you the most beautiful gift. Acceptance.
But what significance did those digital decimal points really have, anyways? While I understood my allergist to be the expert on the topic, my survival instincts blinded me with skepticism. After steering clear of tree nuts for twenty-four years as if my life depended on it (Because, it did), how could I place enough trust in these numbers to unravel the strict avoidance I’d maintained for two decades?
Well, knowledge is power.
What is Immunoglobulin E?
Immunoglobulin E (IgE) represents a category of antibodies produced by the immune system. When the body encounters a potential allergen, it can generate allergen-specific IgE antibodies, initiating what is known as the sensitization process. Upon subsequent exposure to the same allergen, these antibodies attach to the immune cells in the body, prompting the release of histamine chemicals into the bloodstream. This process constitutes the underlying mechanism of an allergic reaction.
The presence and concentration of these antibodies can be measured through simple scratch tests and/or bloodwork, making IgE testing a common ingredient of allergic syndrome diagnostics.
Skin prick testing, or scratch testing, involves the introduction of a small amount of allergenic substance into the skin. Generally performed on the back or inner forearm, the test takes about fifteen minutes and can offer immediate, in-office results. Sensitivity to the allergen is measured by hive, or wheal, size in millimeters. Physicians have the ability to test for nearly 150+ allergies using skin testing, but the method is not recommended for those with severe skin conditions, like eczema or dermatographia. And, it’s likely you’ll be walking out of the office with a slathering of antihistamine cream across the testing site.
A standard blood draw can detect the concentration of allergen-specific IgE antibodies in the bloodstream, measured in kilounits of allergen-specific IgE per liter (KUA/L). The number of allergens that can be evaluated through serum testing is more limited, and the results tend to have a longer turnaround time from the laboratory. Although this assessment is more expensive, it carries only one needle prick and leaves behind the risk of itching.
Both tests are accompanied by their own merits, offering the provider and patient with greater insight into allergic conditions. The two may be used independently or in combination with one another, but should not be ordered until a convincing history of potential IgE-mediated symptoms has been established.
Allergic Nuance
Throughout childhood, I had no concept of this diagnostic process. I attended the appointments, suffered through the needle pricks, and then simply adhered to whatever my allergist prescribed. Epinephrine, strict avoidance… Allergies felt binary – Either I was allergic to something, or I was not. But this rudimentary understanding ignored many of the intricacies of food allergy diagnostics.
It wasn’t until I had the adult responsibility of monitoring my own electronic medical records that I grew curious of the vague numbers that populated within it. And take it from me – The girl who unexpectedly encountered a slew of zeros across her chart at age twenty four – Allergy testing is much more nuanced than we have been made to believe.
Let’s debunk some of these misconceptions.
Myths of IgE Testing
Myth: IgE testing is diagnostic.
Nope! Blood serum and skin prick testing are popular and powerful tools, but they are not independently diagnostic. A review of medical history and past symptomatology can better inform the collected IgE results, but a double-blind oral food challenge is consider the “gold standard” for diagnosing food allergies.
Myth: A positive IgE test result means that you are allergic to that food.
Not exactly. According to FARE, blood and skin prick tests yield a 50 – 60% false positive rate, meaning that tests can indicate that you have an allergy to something that you are not actually allergic too. This partly informs why IgE tests are not diagnostic, and results should be interpreted in the context of other findings.
According to an article in the Journal of Pediatrics, “Another primary reason for misdiagnosis is a lack of understanding of what the results of serum IgE testing truly mean. In the absence of clinical IgE-mediated symptoms with ingestion of the food, a positive serum IgE test to that food merely means a patient is sensitized to it…. The key to the diagnosis of food allergy cannot be overstated; it begins with a detailed clinical history and then physical examination.” Past symptomatology matters!
Myth: All blood tests are created equally.
Not true. Allergen-specific IgE serum testing looks at whole allergens, while component testing looks at individual allergen proteins. Using this technology, component testing can specify which specific proteins in the allergen you are sensitive to. For more on this topic, check out my personal experience with component testing in a recent collaboration with Allergy Insider and Spokin: Allergy Component Testing: Alyssa’s Story.
Myth: IgE blood testing can predict the severity of a potential allergic reaction.
Wrong again! IgE levels cannot predict the severity of a potential allergic reaction. This was clearly articulated by Fleischer & Burks (2015), who wrote “Many individuals wrongfully correlate the food-specific IgE level with the probability and/or severity of reacting to that food.” Instead, IgE levels represent sensitivity, or the likelihood that the allergy exists. IgE blood work simply measures the concentration of antibodies present in the bloodstream, rather than allergic thresholds.
Myth: IgE testing is affected by antihistamine medications.
Yes, and no. According to FARE, IgE blood testing is not affected by antihistamines. However, skin prick testing is, and your allergist may recommend you stop taking those medications several days before your scheduled appointment.
Myth: Immunoglobulin E (IgE) is exclusive to allergic syndromes.
It’s true that this type of testing cannot diagnose intolerances or food sensitive, but that certainly does not make it exclusive to IgE-mediated allergies. IgE plays a role in the body’s natural defense system against parasites, autoimmune diseases, and other medical conditions.
Updated Bloodwork
Having learned my lesson last visit, I am now committed to following up with my allergist every two years for updated bloodwork. In August of 2023, I braved my needle phobia and had the lab run a full food and environmental allergy panel. Thankfully, a more complete understanding of Immunoglobulin E helped me better interpret the results received at that appointment.
In childhood, I was prescribed strict avoidance of peanuts, tree nuts, fish, and legumes. Repeated testing revealed that between the ages of 18 and 24, my tree nut and fish antibodies seemed to naturally dissipate – A rare occurrence, but a miracle that I am continually grateful for. My concentration of peanut antibodies followed suit, decreasing from >100.00 KUA/L to 44.7 KUA/L during that same timeframe. Despite the decline, component testing confirmed that I was still very much allergic to the individual peanut proteins responsible for severe reactions.
Fast forward to August of 2023, two years and an anaphylactic reaction later, peanut has shot back up to >100.00 KUA/L.
Comparison of Peanut IgE Levels at Ages 24 and 26
Honorable mention goes to cats, dogs, dust, and cockroaches, who all fell in the 5 – 10 KUA/L range. A more comprehensive list of my past results is linked in my blog post here.
My immediate reaction to the spiked levels was clouded by fear – My allergy is getting worse?! Well, maybe not. Keeping the ABCs of IgEs in mind, this number does not represent the severity of my food allergy, nor does it predict the severity of a potential allergic reaction. Rather, it simply measures the concentration of antibodies in my bloodstream.
Okay, but did my recent allergic reaction skyrocket the antibodies? Well, it seems like the jury is still out on that one. According to a 2016 study published in the Journal of Allergy and Clinical Immunology Practice, accidental exposure to milk, egg, or peanut that resulted in allergic reactions in children was not associated with significant increases in wheal size or allergen-specific IgE levels. However, in more recent study published in Clinical and Experimental Allergy, IgE levels specific to the ingested allergen increased following an anaphylactic reaction.
Does anyone have further insight into this connection? I’m quite interested in researching further.
But until then, everything else is still sitting pretty at ‘Undetectable?’ Great! I’ll check back in two.
Rehimini, S., Gabrielli, S., Langlois, A., Clarke, A., De Schryver, S., McCusker, C., Bretholz, A., Zhang, X., Shand, G., and Ben‐Shoshan, M. (2021). Clinical and Experimental Allergy, 51 (2), 364-368.
Sicherer, S., Wood, R., Vickery, B., Perry, T., Jones, S., Leung, D., Blackwell, B., Dawson, P., Burks, A., Lindblad, R., & Sampson, H. (2016). Impact of Allergic Reactions on Food-Specific IgE Concentrations and Skin Test Results. J Allergy Clin Immunol Pract, 4(2), 239-245.
Disclaimer: The content of this post is for educational purposes only, and should not be substituted for medical or professional advice. Please consult with your doctor for more information.